Why postmenopausal uterine hypertrophy?
summary
Uterine hypertrophy can be classified as a gynecological disease, generally refers to the patient's uterus uniform enlargement, muscular hypertrophy up to 2.5 to 3.2 cm. The basic pathological manifestation of the disease is the change of vascular wall and smooth muscle cells in the myometrium. Uterine stiffness increased, uterine artery and vein dilated obviously, elastic fiber hyperplasia appeared around the new blood vessels, accompanied by varying degrees of bleeding. The main clinical manifestation is the increase of leucorrhea, in addition, there may be perineal distension or lumbosacral pain. Now let's talk about it.
Why postmenopausal uterine hypertrophy?
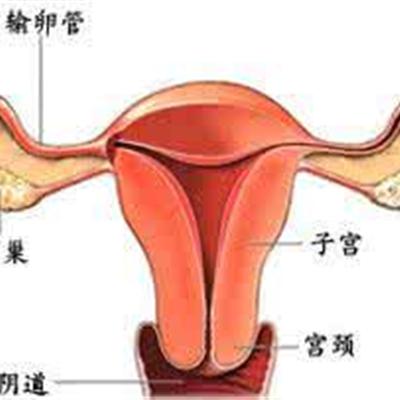
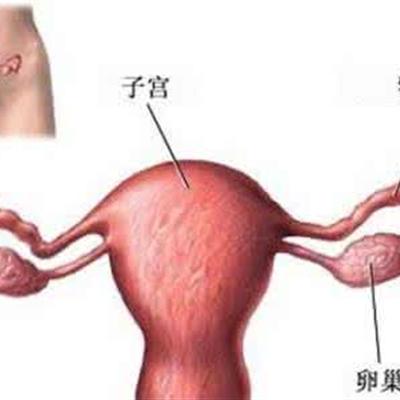
* 1: the main causes of cervical hypertrophy usually include: (1) mucus retention may occur in the deep part of the cervical gland, forming a cyst of different sizes, causing cervical hypertrophy. 2) Chronic inflammation of the uterus long-term stimulation, make cervical edema, hyperemia, cervical stroma and gland hyperplasia and cause cervical hypertrophy.
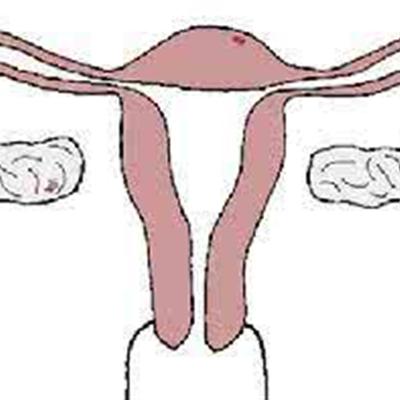
Second: the patients with uterine hypertrophy are mostly multiparous women. Some patients have a long illness time and a large amount of bleeding, which can lead to anemia. Generally, the uterus can be enlarged to the size of 6-week pregnancy, and the texture is generally tough due to the proliferation of fibrous connective tissue. Some patients also have bilateral ovarian enlargement, multiple follicular cysts.
Third: uterine hypertrophy generally does not need treatment, if patients with erosion, cervical erosion can be treated with potassium dichromate solution, 10% iodine or 10 ~ 30% silver nitrate solution for smear. For those with deep and extensive erosion involving cervical canal or malignant transformation, cervical conization can be performed and pathological analysis can be made.
matters needing attention
As the causes of uterine hypertrophy are more diverse, patients can take measures to prevent its occurrence, such as strict adherence to family planning, prevention of postpartum infection and postpartum uterine contraction in patients with poor should be timely application of uterine contraction drugs. Postpartum appropriate exercise, in order to prevent the occurrence of uterine retroversion, as soon as possible to reduce pelvic congestion. If there are symptoms, active treatment should be taken to avoid the continuous stimulation of estrogen and so on.

















