What are the symptoms of hip dislocation?
summary
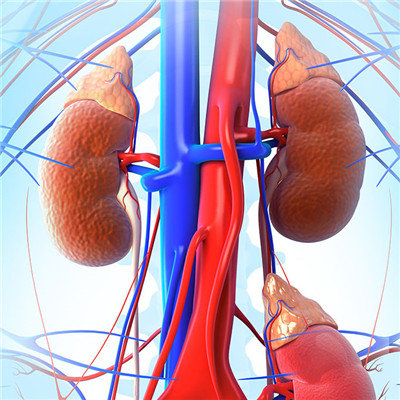
The hip joint is a pestle and mortar joint, with tough ligaments and strong muscle flaps around it, so it is very stable. It is only under the action of indirect violence that it dislocates through the weak area between ligaments. Most of them are young and middle-aged people who are injured by the impact of strong violence in labor or traffic accidents. Dislocation of the femoral head behind the Nelaton line is posterior dislocation; The former is anterior dislocation. Torsion, leverage, or conducted violence can be caused. However, the femoral head impacted the bottom of acetabulum and prolapsed into the pelvis due to conduction force, which belongs to central dislocation. What are the symptoms of hip dislocation? Let's talk about it
What are the symptoms of hip dislocation?
Subluxation is often not eliminated due to factors hindering reduction. The X-ray showed false appearance, carelessly changing plaster, too large anteversion angle or acetabular dysplasia, so even after reduction, it was easy to redistribute. There was a history of trauma, pain and limited activity. The affected limb was shortened, and the hip joint showed flexion, adduction and internal rotation deformity. The prolapsed femoral head can be felt in the buttocks, and the greater trochanter moves up obviously.

The complications of avascular necrosis of the femoral head are mainly due to rough manipulation or excessive surgical trauma, which damage the blood supply of the femoral head; When fixed, the strength is extremely abducted; Before reduction, the traction was not enough or the adductor and iliopsoas muscles were not released, and the femoral head was over compressed after reduction.

Hip osteoarthropathy is a late complication, generally in older children after surgery, to adulthood is often difficult to avoid similar complications. Epiphyseal separation of the femoral head, fracture of the upper femur, sciatic nerve injury, etc. These are caused by insufficient traction, the use of violence or too shallow anesthesia during reduction, which can be generally avoided.
matters needing attention
Posterior dislocation of the hip can be reduced by manual reduction, with few difficulties. The reduction method is stable and reliable with hip flexion and knee flexion traction along the femoral axis. The method of allis is supine traction, and the method of Stimson is prone traction. When repositioning, the manipulation should be slow, the traction force should be used continuously, violence or sudden turning is strictly prohibited, and the forced torsion is not allowed when there is resistance. If the traction technique is invalid, you can use "rotation" Question mark technique.