Can congenital rectum and peripheral organ fistula be cured?
summary
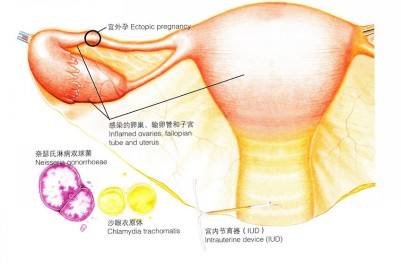
Congenital rectal and peripheral organ fistula refers to the incidence rate of anorectal malformation in neonates, which is about 1:1500 to 5000. Half of the patients had fistula. The common fistulas were rectoperineal fistula and rectovaginal fistula; The rare is congenital rectum and surrounding organ fistula, such as rectovesical fistula, rectourethral fistula, rectovaginal fistula, etc. Can that congenital rectum and around viscera fistula be cured?
Can congenital rectum and peripheral organ fistula be cured?
Clinical symptoms: when anorectal malformation combined with fistula, meconium can be seen discharged from urethra and vaginal fistula respectively. Meconium discharge is not smooth, can have low intestinal obstruction symptoms. Rectovaginal fistulas usually open in the fornix of the posterior vaginal wall, and there is no local sphincter to control feces, which is easy to cause reproductive system infection. Rectovesical (urethral) fistula can cause urinary tract infection.

The cause of the disease is that the differentiation of mesoderm and endoderm is obstructed in the embryonic stage, and the cloacal space is not completely separated during the development, resulting in the formation of fistula between rectum and surrounding organs. Rectourethral fistula, see feces from the urethra, not mixed with urine. If feces and urine mixed discharge for rectovesical fistula. The excretion of feces from vagina is rectovaginal fistula or rectovaginal fistula.

All of them need surgical treatment. Rectovesical fistula is often associated with urinary tract infection and should be operated early. If the defecation of other types of fistula is unobstructed, the operation can be delayed until 3-5 years old. Transabdominal or perineal resection of the fistula, rectal pull down suture in situ, or anal sphincteroplasty.

matters needing attention
The timing of operation should be carefully selected, and immediate operation should be avoided due to the urgent needs of patients. Surgery should wait for all inflammation to subside and scar to soften, 3 months after injury or repair. If the fistula is large, it will take six months. At the same time, all inflammation must do appropriate drainage.