How long can fourth ventricle tumor live?
summary
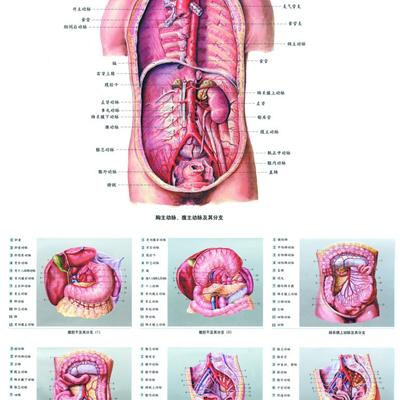
Due to the complex anatomical structure of the fourth ventricle, which is closely related to the brain stem and other life centers, the surgical treatment of tumors in this region is difficult. The course of disease is generally 3 years, clinical manifestations: headache, dizziness, walking instability, vomiting, dysphagia. Signs: papilledema, cerebellar ataxia, pharyngeal reflex weakened. Next, I'd like to share with you how long can the fourth ventricle tumor survive?. Hope to help you.
How long can fourth ventricle tumor live?
First, after general anesthesia, the patient was placed in prone position or lateral prone position. In case of acute onset and hydrocephalus, craniotomy was performed through right occipital angle puncture and external ventricular drainage first, and craniotomy was performed through suboccipital posterior median approach to open the foramen magnum to form 4 cm ~ 5 cm × 3 cm ~ 4 cm bone window, cerebellar tonsillar hernia or tumor protruding into the cervical spinal canal, biting open the ring vertebra to expose and decompress.

Second, under the microscope, the dura mater was cut in a "Y" shape, the cerebellomedullary cistern was opened, the brain automatic traction device was placed after slow decompression, and the boundary between the tumor and the lateral wall of the fourth ventricle was separated along the tumor edge through the inferior cerebellar vermis approach or the cerebellomedullary fissure (meningeal sail) approach, and the tumor feeding artery of the posterior inferior cerebellar artery branch was searched, and the tumor was cut off by electrocoagulation. If the tumor adheres closely to the dorsal side of the brainstem at the base of the fourth ventricle and is difficult to separate, a thin layer of tumor or capsule should be left to avoid affecting the brainstem function. In all cases, the outlet of midbrain aqueduct was opened under microscope to avoid postoperative hydrocephalus.

Third: close hemostatic tumor bed, covered with hemostatic gauze. When the tumor of the fourth ventricle is large, most of them are combined with hydrocephalus, and excessive loss of cerebrospinal fluid causes intraventricular pneumatosis. Therefore, normal saline should be perfused at the end of the operation. It can not only prevent the loss of cerebrospinal fluid, but also prevent the postoperative supratentorial intraventricular hematocele caused by blood reflux. Those with poor exposure can be treated with neuroendoscope assisted microsurgery via the median posterior fossa approach; Microsurgery was performed through cerebellomedullary fissure vermis approach. In the endoscopic group, 30 cases were used to separate the top, back and lateral part of the tumor ° The operation was performed under direct vision; When changing the operation position, it is necessary to observe and distinguish the structure again before operation.

matters needing attention
After the operation, the dura mater was sutured and suspended. If there was more leakage of cerebrospinal fluid, gelatin sponge and ear brain glue were used to repair the leakage. The drainage tube was placed outside the dura mater, and the scalp was sutured tightly. Routine perioperative management and comprehensive treatment were performed according to the pathological results.